Preservative Efficacy Testing Vs. Ethylene Oxide Residuals Testing
What are preservatives and Ethylene Oxide Gas (EtO)?
Preservatives and ethylene oxide gas relate for some medical products, drugs, and cosmetics. Preservatives are substances mixed into creams, gels, and other liquids. Preservatives are used to prevent the growth of bacteria, fungi, and other microorganisms within a medical, cosmetic, household, or food product. Preservatives also help keep the freshness of the appearance of a product and keep its consistency intact over time. Preservatives in baby wipes, cosmetics, vials, and other products must undergo preservative efficacy testing to prove the preservative’s antimicrobial function. Preservative efficacy testing is also called preservative challenge testing. Ethylene oxide (also called EO or EtO) is a chemical gas commonly used to sterilize medical devices and products. Ethylene oxide gas is a potent and highly penetrating alkylating agent. These characteristics make ethylene oxide sterilization extremely effective. Indeed, the primary ethylene oxide uses are sterilization despite ethylene oxide’s carcinogenic effects on humans. Thus, it is critical to find labs that do ethylene oxide residual analysis so that medical devices and products sterilized with ethylene oxide can limit patient ethylene oxide exposure. This article covers ethylene oxide residuals testing as well as preservative efficacy testing (e.g., preservative testing for cosmetics and lotion preservative testing).
What is preservative efficacy testing (PET)?
Preservative efficacy testing, also known as preservative challenge testing, determines the effectiveness of a preservative during its shelf life and evaluates how well a product withstands microbial contamination during use. Preservative testing for cosmetics and lotion preservative testing are common preservative efficacy evaluations.
What is Ethylene Oxide sterilization?
As mentioned above, ethylene oxide gas is an extremely effective sterilizing agent. However, ethylene oxide effect on humans can be toxic. Sterilization by ethylene oxide kills microorganisms through exposure to ethylene oxide gas under vacuum and humidity. Ethylene oxide gas is used either as one hundred percent ethylene oxide, a carbon dioxide/EtO mixture, or a mixture with other gasses. While ethylene oxide is useful as a sterilizing agent, at certain levels, ethylene oxide effects on humans can be deadly over time. Indeed, exposure to certain levels of ethylene oxide gas is capable of causing cancer. The cancer-causing risks of ethylene oxide sterilization are why the FDA requires ethylene oxide residual analysis.
What is ethylene oxide residuals testing And Ethylene Oxide Exposure?
The primary issue with using ethylene oxide effects on humans is its absorption into certain materials and its reaction with water or other material components to form toxic residual compounds (ethylene oxide, ethylene glycol, and ethylene chlorohydrin). Exposure to ethylene oxide and ethylene oxide residual compounds is hazardous both to people and to the environment. Ethylene glycol is formed from ethylene oxide and water reaction, while ethylene chlorohydrin is formed from the interaction of ethylene oxide and chloride compounds. Thus, dangerous ethylene oxide effects on humans can come from ethylene oxide’s residuals not just ethylene oxide itself. Products sterilized with ethylene oxide must meet strict ethylene oxide residuals limits during ethylene oxide residual analysis to keep patients safe during medical device and product use. Ethylene oxide residual analysis assesses medical devices and other ethylene oxide sterilized products or packaging for their residual ethylene oxide and ethylene chlorohydrin content.
How common is ethylene oxide sterilization?
Approximately 20 billion medical devices are sterilized with ethylene oxide each year. Thus, ethylene oxide sterilization accounts for about half of sterilized medical supplies in the United States. As a result, ethylene oxide effects on humans and ethylene oxide residual analysis are a priority for companies that use ethylene oxide for device sterilization.
What products require preservative efficacy testing?
Preservative efficacy testing can be used to determine the best preservative to use in your topical formulation and the minimum effective concentration needed to preserve the pharmaceutical, food, or biotechnology product being assessed. Topical formulations (gels, creams, ointments, and lotions) comprise a water or oil base that delivers various medications, natural substances (such as herbs), or moisture through the skin. Topical cosmetics contain preservatives to support the stability of the formulation and prevent microbial growth during repeated product use. Preservative challenge testing is also used for parenteral products containing multiple doses. In parenteral products, antimicrobial preservatives inhibit the growth of any microorganisms introduced during repeated insertion and withdrawal to load individual amounts.
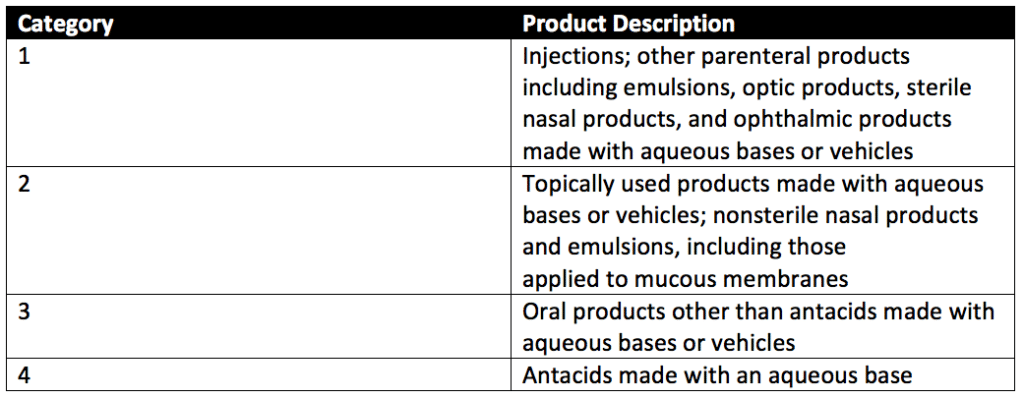
Preservative testing can evaluate four categories of products. Lotion preservative testing falls under Category 2, while parenteral product testing falls under Category 1 testing. The preservative testing product categories are detailed in Table 1 of USP 51, reproduced below.
What products require ethylene oxide (EtO) residuals testing?
Any items sterilized using ethylene oxide require ethylene oxide residuals analysis. Due to its low-temperature conditions, ethylene oxide sterilization is well suited for medical devices with embedded electronics and medical devices that cannot withstand steam (autoclave) sterilization. Ethylene oxide is also used to sterilize the personal protective equipment and drapes used by doctors and healthcare workers. Medical device types that are sterilized with ethylene oxide range from external wound dressings to implantable stents. Other devices include heart valves, vessel closure devices, catheters, and guidewires. Products combining devices, drugs, and biologics within a single item may also be sterilized using ethylene oxide.
Ethylene oxide can sterilize almost every type of plastic. Standard materials sterilized with ethylene oxide are plastics, heat-labile materials (e.g., electronics), elastomer polymeric materials, and biomaterials.
Ethylene oxide is not recommended for medical devices with embedded batteries due to the vacuum used during sterilization. Ethylene oxide sterilization is not recommended for materials sensitive to temperatures ranging from 30°C to 60°C or for medical devices made with materials that are sensitive to humidity. Polymers that are resistant to ethylene oxide sterilization are polyolefin resins such as polypropylene (PP), high-density polyethylene (HDPE), and low-density polyethylene (LDPE). Resistant polymers require additional exposure to ethylene oxide and often exceed ethylene oxide residuals limits after ethylene oxide residual analysis.
How is preservative testing performed?
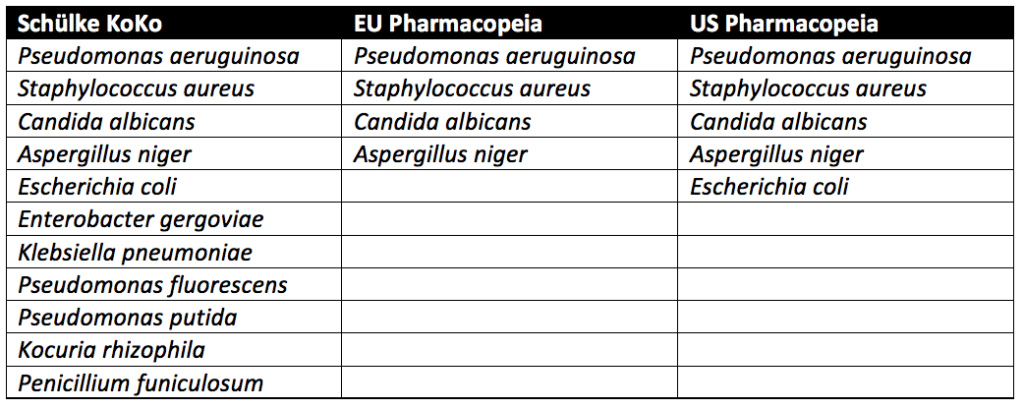
Three approaches are used in preservative testing for cosmetics, lotion preservative testing, and preservatives testing of other products. These approaches come from the Schülke KoKo Test, United States Pharmacopeia (USP), and the European Pharmacopeia.
Schülke KoKo Test vs. U.S. Pharmacopeia vs. European Pharmacopeia
Pseudomonas aeruginosa, Staphylococcus aureus, Aspergillus niger, and Candida albicans must be tested for in all cosmetic products sold in the European Union (EU). Thus, lotion preservative testing and preservative testing for cosmetics must pass exposure to Pseudomonas aeruginosa, Staphylococcus aureus, Aspergillus niger, and Candida albicans to be sold in the EU. In addition to the microbes above, testing with microbes known to lead to spoilage of cosmetic products is recommended but not required. In the United States, the USP guidelines require testing of Escherichia coli in addition to Pseudomonas aeruginosa, Staphylococcus aureus, Aspergillus niger, and Candida albicans. Spoilage microbes are not needed for PET. In contrast to the pharmacopeia tests, which only evaluate pathogenic microbes, the Schülke KoKo test evaluates product spoiling microorganisms. Schülke KoKo test’s spoiling microorganisms are based on decades of preservatives testing for cosmetics experience from Schülke & Mayr in Germany.
USP preservative efficacy testing evaluates cosmetic products by exposing them to a single microbial strain at a time. Additional details on USP preservative challenge testing, which follows similar procedures to the European Pharmacopeia, can be found through reading our articles on Preservative Challenge Testing And USP 51 and Preservative Efficacy Testing For Medical Devices. In contrast, for the Schülke KoKo test, the single cultivated microbes are brought together into a mixed suspension to challenge the cosmetic product. A new mixed suspension is prepared for each of the six inoculation cycles for Schülke KoKo testing. Since the Schülke KoKo test uses a mixed microbe inoculation, it simulates microbial exposure of a product during production, filling, and use. Indeed, a product would likely be exposed to multiple microbes at once instead of one at a time. Overall, though different from the USP and European Pharmacopeia methods, the Schülke KoKo Test is a reliable test method for preservative testing for cosmetic products and lotion preservative testing.
First, cultures of Candida albicans (ATCC No. 10231), Aspergillus brasiliensis (ATCC No. 16404), Escherichia coli (ATCC No. 8739), Pseudomonas aeruginosa (ATCC No. 9027), and Staphylococcus aureus (ATCC No. 6538) are prepared. Stock cultures of these organisms are prepared by centrifuging an ATCC culture removing residual media from the prior culture and resuspending the microorganisms in a sterile suspension fluid. The suspension fluids for each microorganism referenced above are prepared at a microbial count of about 1 × 108 colony-forming units per milliliter (CFU/mL).
Preservative testing for cosmetics is performed in five sterile, capped containers. Suppose the product’s original container is sterile, can be entered aseptically, and holds an appropriate product volume. In that case, the original filled product containers may be used. Each of the five product samples is injected with a test suspension of either Candida albicans, Aspergillus brasiliensis, Escherichia coli, Pseudomonas aeruginosa, or Staphylococcus aureus. Each product sample is exposed to only a single microbe of the five listed, and all microbes are exposed to the product during testing. The microbial test suspension injected is between 0.5%- 1% of the volume of the product under assessment and is at a concentration of 1 × 105 and 1 × 106 CFU/ml of the product for category 1-3 products. The final concentration per ml of category 4 products is between 1 × 103 and 1 × 104 CFU/mL.
Each of the five product samples (for cosmetic, parenteral, or lotion preservative testing) with their respective microbial injections is incubated at a simulated room temperature of 22.5 ± 2.5°C or 32.5 ± 2.5°C depending upon the microbe the product sample is exposed. Microbial counts are taken at 7, 14, and 28 days for most microorganisms tested. The plate-count method determines the number of CFU present in each inoculated product sample. This plate-count method is completed in duplicate. Once all counts are taken, the change in log10 of the concentration of CFU/ml is calculated for each microorganism. The requirements for antimicrobial effectiveness are met if no increase in microbial growth for the various organisms tested occurs within the timeframes specific to each organism. are met. No increase in microbial growth is defined as not more than 0.5 log10 units more than the previous microbial growth value.
How is ethylene oxide (EtO) residual testing performed?
As mentioned earlier, products sterilized with ethylene oxide must meet strict EtO residuals limits to mitigate ethylene oxide effects on humans and prevent patients from product-related illnesses. EtO sterilized materials vary in their ability to absorb, retain and release ethylene oxide (EtO). If your device or product isn’t in physical contact with the patient, there is no need to perform EO residual testing. However, if your device is in contact with the patient, EtO sterilized devices are placed into one or more of three exposure categories based on the duration of contact a medical device has with a patient. These categories are designed to protect patients against EtO-related cellular toxicity that can cause varying degrees of illness and tissue damage. The categories of EtO exposure are limited exposure (less than 24 hours), prolonged exposure (1 day to 30 days), and perpetual exposure (lifetime limit). Each category has specific limits (in milligrams) that must be met.
Two different analysis methods for EtO residuals are used to determine the amount and type of EtO residuals in your sterilized product. These methods are simulated-use and exhaustive extraction. Evaluation of a product via either simulated-use or exhaustive extraction is sufficient to meet the ISO 10993-7 standards for EtO residual testing. Evaluation of a product via both simulated-use and exhaustive extraction is not necessary.

How is simulated-use ethylene oxide extraction performed?
ISO 10993-7 states that simulated-use extraction evaluates “residue levels available to the patient or user from devices during the routine use of a device with water extraction to simulate product use.” This extraction method is used when only part, not the entire EtO sterilized device, will be in contact with a patient. Thus, the simulated-use extraction will simulate the exposure of a patient to the fraction of the EtO sterilized device that the patient would interact with during normal product use. For large, surface-contacting devices (such as drapes or gowns), the EtO residual transferred to the patient may be estimated with a transfer reduction factor approach. The transfer reduction factor approach may be based on weight or surface-area-proportion basis (Annex E of ISO 10993-7).
How is exhaustive ethylene oxide extraction performed?
ISO 10993-7 states that exhaustive extraction involves the extraction of EtO “until the amount of EtO or ECH in a subsequent extraction is less than 10 % of that detected in the first extraction, or until there is no analytically significant increase in the cumulative residue levels detected.” This extraction method is best used when the entire device will be in contact with a patient and estimates the majority of EtO residual that a patient would be exposed to during device use. Extractions are typically performed every 24 hours until exhaustive criteria, and device use (limited, prolonged, and permanent exposure) criteria are met. For large or complex devices, exhaustive extraction may be impractical. In these instances, extraction of representative portions of the device may be used to extrapolate the EtO residuals for the entire device. If the yield of the first extraction is very small (as is the case with devices with little residue or devices that release analyte at a slow rate), continue extraction until the increase in the cumulative yield of the analyte extracted is small relative to the analytical uncertainties.
What are the differences between preservative efficacy testing and EtO residuals testing?
EtO residuals testing is used for cancer-causing toxin prevention. In contrast, preservative challenge testing determines the best preservative for use and the minimum effective concentration needed to preserve multidose parenteral products, topicals products, food, or other healthcare items that contain preservatives. Together preservative efficacy and cytotoxicity tests ensure that parenteral products, cosmetic products, and medical devices meet the regulatory safety criteria for ethylene oxide residuals toxicity and antimicrobial activity.
Summary
Overall, preservative efficacy testing (PET) and ethylene oxide (EtO) residuals testing are imperative for the regulatory approval of pharmaceuticals, cosmetics, lotions, and medical devices. These tests ensure that parenteral products, topicals, and medical devices are non-toxic and have sufficient antimicrobial activity to keep patients safe during product use. Lotion preservative testing and preservative testing for cosmetics are particularly common PETs because not all parenteral products contain preservatives. All in all, ensure you choose a contract manufacturing organization that can support you with appropriate EtO residuals and preservative efficacy testing for your unique cosmetic, pharmaceutical, or medical device product needs.
MycoScience is a contract manufacturing organization specializing in Preservative Efficacy Testing, EO Residual Testing and sterile syringe and vial filling. MycoScience also offers Bioburden Testing, Cleaning Validations, Microbial Aerosol Challenge Testing, Accelerated Aging, Microbiology Testing, Cytotoxicity Testing, Bacterial Endotoxin Testing, Package Integrity Testing, Sterilization Validations & Environmental Monitoring services medical devices and allied industries. MycoScience is an ISO 13485 certified facility.
References
Bernhard Linke. Sterilization methods and impact on electronics in medical devices. EE Times. July 2011.
International Organization for Standardization. Biological evaluation of medical devices — Part 7: Ethylene oxide sterilization residuals. Geneva (Switzerland): ISO; 2008. (ISO 10993-7:2008).
Michael J. Akers. Sterile Drug Products Formulation, Packaging, Manufacture, and Quality. Drugs and the Pharmaceutical Sciences. Informa Healthcare. 2010.
Purell. Sterilization Of Polyolefins: A Methodological Overview. Lyondell Basell Industries.2011.
United States Food & Drug Administration. Ethylene Oxide Sterilization for Medical Devices. Digital Article. September 2020.
United States Pharmacopeial Convention. <51> Antimicrobial Effectiveness Testing. Rockville, MD, USA. 2021. (USPC <51>).
Sharing this in your social netwroks